Seven Days Inside an Ambulance Drug Safe
救護車藥物保險箱的七天:把看不見的儲存溫度變成數字
This is a field evidence note, not a research report. I keep the full observation, data, method, and the limits of inference — what this data can and cannot support is written into the article itself.
1. The question: do we know what temperature the drugs on the ambulance are actually kept at?
Some EMS systems abroad have dedicated staff who manage the stocking of equipment, consumables, and even medications. EMS in Taiwan has no such staffing — usually one administrator sets the rules, and everyone else uses, restocks, and checks stock accordingly. Items, quantities, and expiry dates — the things that appear on paper — are kept running this way; with current staffing, this is already as much management as can be done.
But there is one variable that never even makes it onto paper: the temperature the drugs actually endure on the ambulance.
And this was never about just one vehicle. How many ambulances across Taiwan have no carport or garage and sit long-term exposed to sun and rain? I don't know the exact number — and as far as I know, no one does. For every vehicle parked like this, the drug-storage environment is equally outside everyone's view.
I have always seen the ambulance this way: it is not just a vehicle, but a mobile workplace. Inside it, personnel perform medical care, patients receive care, and drugs are stored on standby. Once you look at it as a "workplace," many things treated as "vehicle problems" become "environmental management problems" — in a fixed workplace, the drug-storage environment has temperature rules and someone responsible; but this moving workplace, during the majority of the time when it is not on a call and is simply parked outside, has its role as a drug-storage space almost entirely out of sight.
I am not the first to notice this. Colleagues have made similar observations and measurements of prehospital drug-storage conditions, and have presented them as conference posters; but such data is still scattered, remaining the self-initiated action of individual conscientious people, not yet part of any system. I wanted to add one data point with my own vehicle — to turn this invisible variable into a number that can be discussed.
2. Measurement method
| Item | Detail |
|---|---|
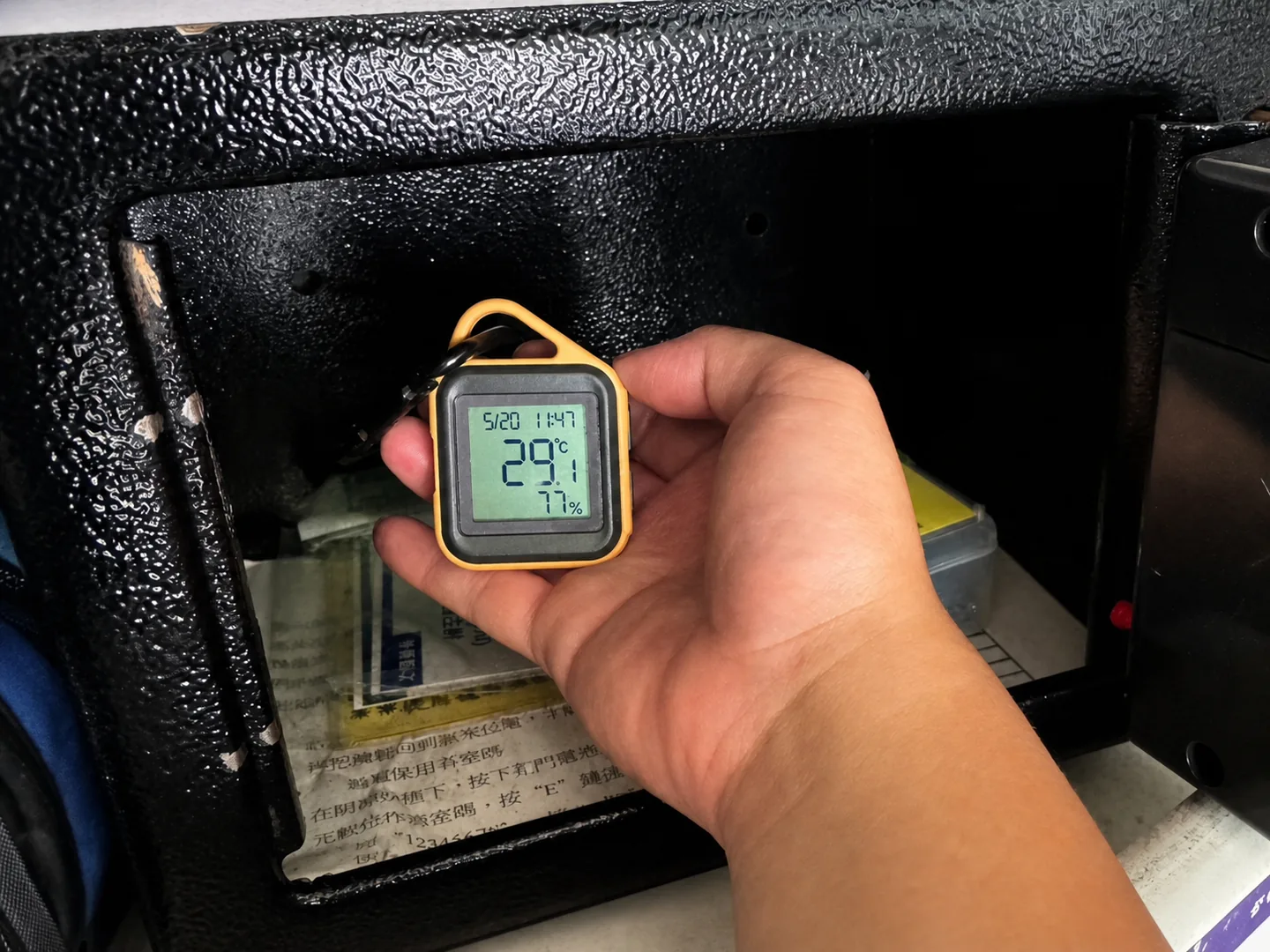
| Subject | One ambulance parked long-term outdoors without shelter; sensor placed inside the drug safe |
| Period | 2026-05-20 12:30 to 2026-05-27 12:30 (about 168 hours) |
| Frequency | Temperature and relative humidity logged every 30 minutes |
| Equipment | PolarBear AT1 consumer-grade temperature/humidity logger (nominal accuracy ±0.2°C, not third-party calibrated) |
| Data volume | 337 raw records; after excluding 1 outlier, 336 valid records |
Outlier handling: at 2026-05-26 09:30 there was one record of 0°C / 0%RH. The records immediately before and after were in the normal range, and temperature and humidity both dropping to zero simultaneously is a typical signature of sensor read failure, so it was excluded. All statistics are computed on the 336 valid records.
Humidity was also fully logged, but this article makes no analytical claim about humidity, leaving it for later when there is a clear question to pursue.
3. Findings
Over seven days, peak temperature 41.4°C; above 25°C 91.1% of the time.
| Threshold | Records | Share | Approx. hours |
|---|---|---|---|
| > 25°C | 306 / 336 | 91.1% | about 153 hours |
| > 30°C | 110 / 336 | 32.7% | about 55 hours |
| > 35°C | 18 / 336 | 5.4% | about 9 hours |
| > 40°C | 6 / 336 | 1.8% | about 3 hours |
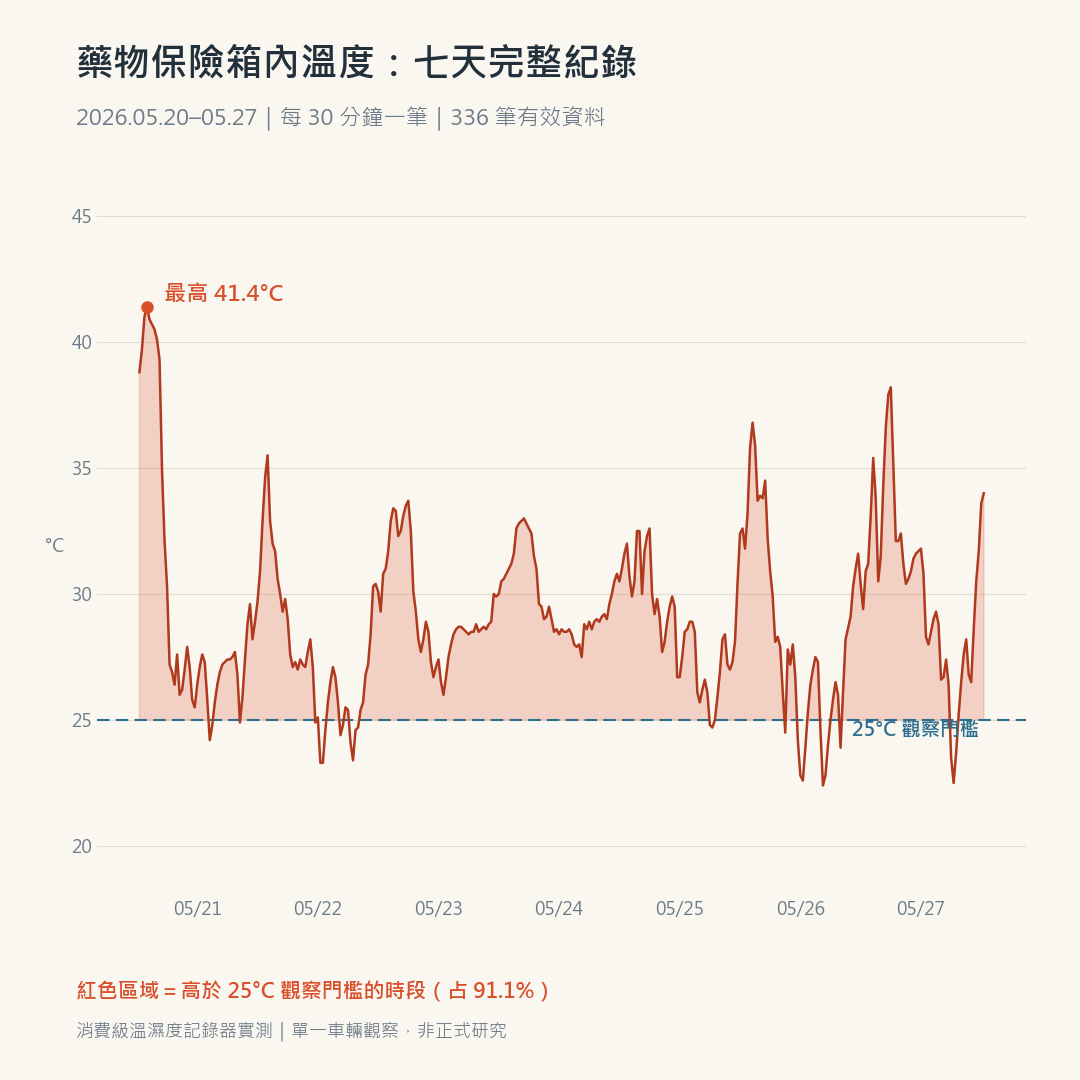
About the 25°C line: this article uses 25°C as an observation threshold. This value has two reference layers: the U.S. Pharmacopeia (USP) defines "controlled room temperature" as 20–25°C, and many injectable drugs use this as the upper storage limit; public drug data from Taiwanese hospitals carry the same requirement — for example, the Kuang Tien General Hospital drug-lookup system records the storage condition for Midazolam injection as "store in a dry place at 15–25°C." The manufacturer labeling for the drugs actually carried on the monitored vehicle will be added once a publicly citable version is obtained; until then, 91.1% should be understood as "above the observation threshold set here," not "above the labeled limit of a specific product."
4. Supplementary observation: inside the safe vs. outdoor air temperature (full seven days)
I paired the full seven days of 336 valid records with regional outdoor air-temperature model estimates for the Tucheng area from the Open-Meteo Historical Weather API; the hourly outdoor data was aligned to the 30-minute in-safe records by linear interpolation.
The full seven-day supplementary comparison shows: the temperature inside the safe was at most 10.0°C higher than the outdoor air-temperature model estimate; the largest gap occurred at 2026-05-20 16:00, when inside the safe was 40.1°C and the outdoor model estimate was 30.1°C.
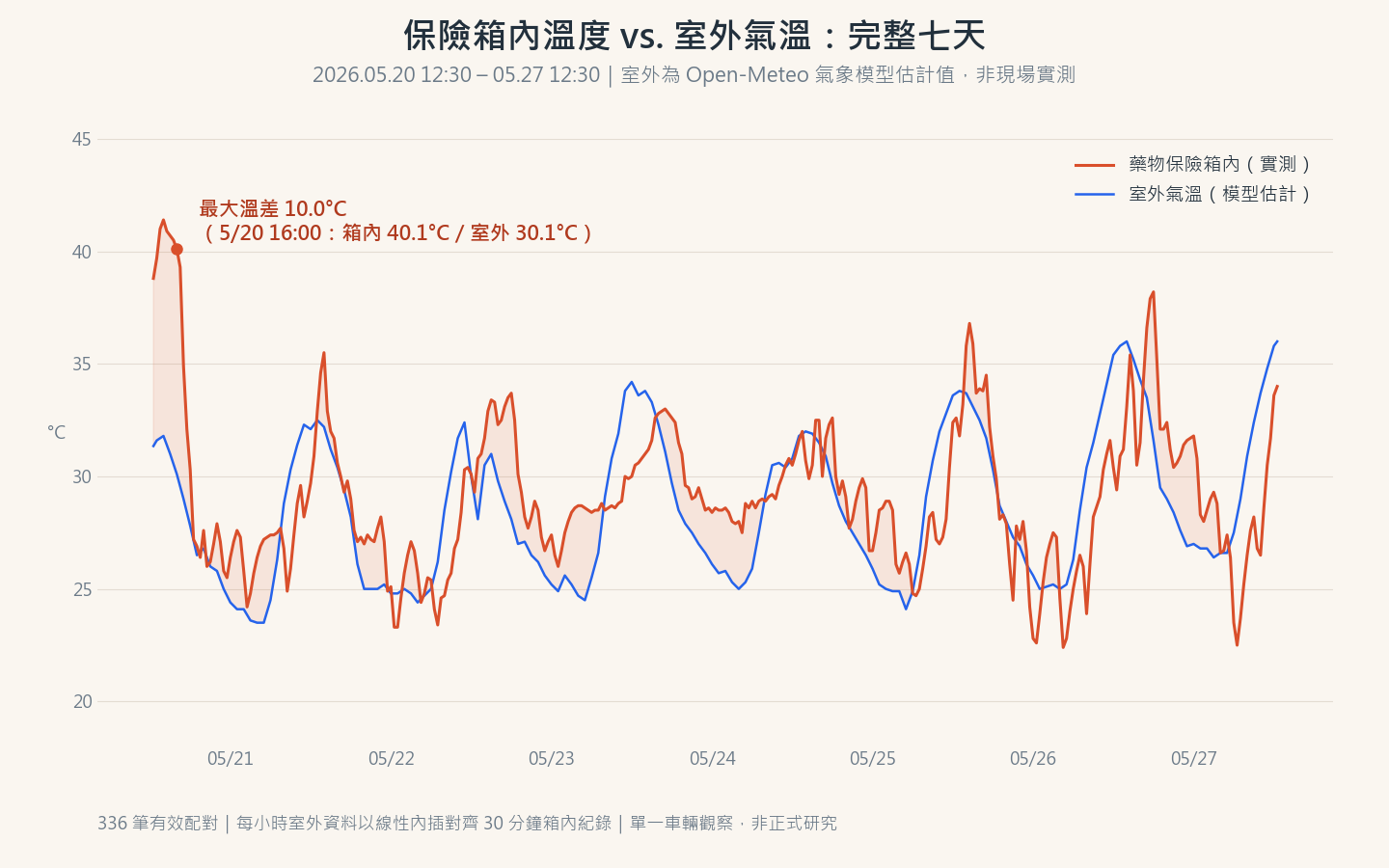
This is still a supplementary observation: the outdoor value is a regional weather-model estimate, not an on-site measurement beside the monitored vehicle, so not every gap can be read as the precise heating effect of the vehicle body. But it is enough to show: the temperature inside the safe is not the same as the regional air temperature at the time. The "33°C today" figure in the news is not the figure the drugs actually endure.
5. Interpretation: the problem isn't "the heat," it's "not yet being routinely monitored"
This data supports only one conclusion, but I believe it is already important enough:
In this vehicle, during this one week, the drug-storage environment deviated from common storage thresholds for over ninety percent of the time — and if no one had actively placed that logger, this number would not exist.
Whether the drugs have degraded requires potency testing to answer, which this data cannot do. But "cannot confirm" is itself a quality-management gap: we are meticulous about expiry dates, yet have no routine data on storage temperature. The premise of an expiry date is that the drug was kept under the conditions required by its labeling — and right now that premise relies not on a system, but on the self-initiated measurement of individual conscientious people.
Those who have measured all see something similar. The difference is that these observations are isolated from one another, never accumulating into a systematic basis for management.
Switch the setting and the gap becomes clear: the same batch of drugs in a hospital pharmacy faces temperature monitoring and recording that is, at minimum, a regulatory and accreditation requirement; move it onto an ambulance and that requirement effectively disappears. I do not mean to assert how thoroughly the hospital side actually complies — but the very presence or absence of the requirement is the gap. The ambulance is a mobile workplace, and the environmental management a workplace should have shouldn't be discounted just because it has wheels.
So what this note really points to is not the one vehicle I measured, but every ambulance across Taiwan that has no carport or garage and is parked outdoors long-term. Their numbers may not match what I measured — but the fact that "no one knows" is the same.
6. Limits of inference
- This cannot say the drugs have degraded. No potency or quality testing was done.
- The temperature figures cannot be extrapolated to all ambulances. Single vehicle, single week, single parking condition. Other vehicles, other seasons, sheltered parking could give entirely different numbers — but "could differ" is exactly the reason more measurement is needed. What can be generalized is not the numbers, but the state: ambulances parked outdoors long-term are equally unmonitored in their storage environment.
- This is not formal research. Consumer-grade sensor, uncalibrated, no control group, no repeated measurement. It is a field evidence note: its function is to raise a question worth taking seriously, not to provide a general answer.
- This is not an accusation of any unit. Long-term outdoor parking has spatial, operational, and practical reasons. This note is concerned with the blind spot at the system level, not the negligence of individual managers.
7. Improvement options: start with the cheap ones
- Establish a baseline: place one temperature logger at the drug-storage location. A few hundred NT dollars, zero administrative burden — turning "don't know" into "know." This is the premise for everything that follows.
- Environmental adjustment: shading, parking location, and in-vehicle storage improvements — there are many options, but before baseline data exists, there's no way to judge which one works. An improvement should not shift risk onto the operational workflow; for example, storing drugs in the duty quarters during downtime and carrying them onto the vehicle only when responding could increase delay, the risk of forgetting them, and handover risk, and should not be adopted on temperature grounds alone.
- System level: make storage-environment temperature a routine part of medication management, just like expiry-date management. One level higher: inventory how many ambulances across Taiwan are parked outdoors without shelter long-term — that most basic number is one no one may currently be able to answer.
- Re-measure: after any improvement, measure again and compare the before and after. Only at this step does a single-point observation become a reusable improvement method.
8. If you want to measure your own vehicle
The method is all in section 2: one consumer-grade temperature/humidity logger, placed in the drug-storage location, logging for a week.
I am not the first to measure, and I hope I am not the last. One vehicle's data is an individual case; when scattered observations from many places begin to be compared against one another, it becomes something else.
Acknowledgements: thanks to the two colleagues who helped with the recording, and to the peers who observed this issue before me.
This is a field evidence note. There are 336 valid raw records in total, and all charts are drawn from measured data. Questions about the method or data are welcome.